Introduction
Physical therapy in West Orange for Wrist Issues
Welcome to Optimum Recovery Rehab Physical Therapy & Rehabilitation’s resource to Triangular Fibrocartilage Complex (TFCC) Injuries. Triangular fibrocartilage complex (TFCC) injuries of the wrist affect the ulnar (little finger) side of the wrist.
As the name suggests, the soft tissues of the wrist are complex. They work together to stabilize the very mobile wrist joint. Mild injuries of the TFCC may be referred to as a wrist sprain. Significant disruption of this area through injury or degeneration, however, can cause more than just a wrist sprain. A TFCC injury can be a very disabling wrist condition.
This guide will help you understand:
- what parts if the wrist are involved
- how these injuries occur
- how health care professionals diagnose the condition
- what treatment options are available
- what Optimum Recovery Rehab Physical Therapy & Rehabilitation’s approach to rehabilitation is
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Hand Pain|limit:15|heading:Hear from some of our patients who we treated for *Hand Pain*#
Anatomy
What parts of the wrist are involved?
The wrist is actually a collection of many bones and joints. It is probably the most complex of all the joints in the body. There are 15 bones that form connections from the end of the forearm to the middle of the hand.
The wrist itself contains eight small bones, called carpal bones. These bones are grouped in two rows across the wrist. The proximal row is where the wrist creases when you bend it. The second row of carpal bones, called the distal row, meets the proximal row a little further toward the fingers.
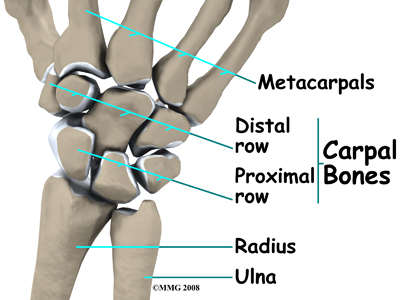
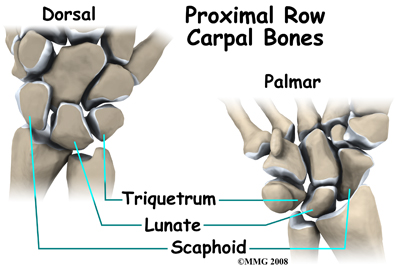
The proximal row of carpal bones connects the two bones of the forearm, the radius and the ulna, to the bones of the hand. On the ulnar side of the wrist, the end of the ulna bone of the forearm moves with two carpal bones, the lunate and the triquetrum.
The TFCC suspends the ends of the radius and ulna bones over the wrist. It is triangular in shape and made up of several ligaments and cartilage. The TFCC makes it possible for the wrist to move in six different directions: bending, straightening, twisting both ways, and side-to-side.
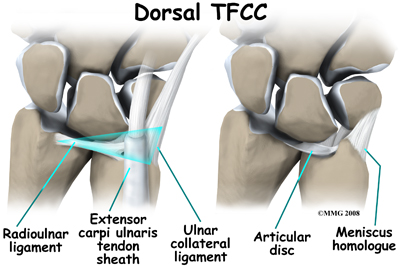
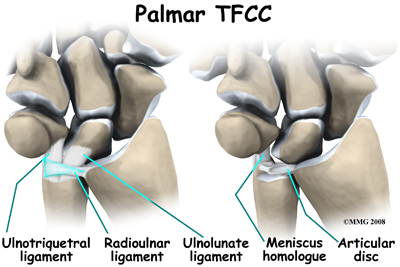
The entire TFCC sits between the ulna and the two carpal bones (the lunate and the triquetrum). The TFCC inserts into the lunate and triquetrum via the ulnolunate and ulnotriquetral ligaments. It stabilizes the distal radioulnar joint while improving the range of motion and gliding action within the wrist.
There is a small cartilage pad called the articular disc in the center of the complex that cushions this part of the wrist joint. Other parts of the complex include the dorsal radioulnar ligament, the volar radioulnar ligament, the meniscus homologue (ulnocarpal meniscus), the ulnar collateral ligament, the subsheath of the extensor carpi ulnaris, and the ulnolunate and ulnotriquetral ligaments.
Injury to the TFCC involves tears of the fibrocartilage articular disc and meniscal homologue. The homologue refers to the piece of tissue that connects the disc to the triquetrum bone in the wrist. The homologue acts like a sling or leash between these two structures.
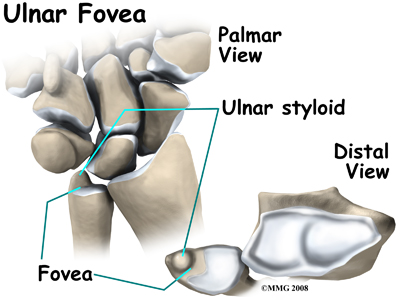
Another important structure to make note of with TFCC injuries is the ulnar fovea. The fovea is a groove that separates the ulnar styloid from the ulnar head. The groove is at the junction of the ulnar bone and wrist. The styloid is a small bump on the edge of the wrist (on the side away from the thumb) where the ulna meets the wrist joint. Later we will talk about the fovea test to diagnose TFCC injuries.
Causes
What causes this problem?
 The TFCC stabilizes the wrist at the distal radioulnar joint. It also acts as a focal point for force transmitted across the wrist to the ulnar side. Traumatic injury or a fall onto an outstretched hand is the most common mechanism of injury. The hand is usually in a pronated or palm down position. Tearing or rupture of the TFCC occurs when there is enough force through the ulnar side of the hyperextended wrist to overcome the tensile strength of this structure.
The TFCC stabilizes the wrist at the distal radioulnar joint. It also acts as a focal point for force transmitted across the wrist to the ulnar side. Traumatic injury or a fall onto an outstretched hand is the most common mechanism of injury. The hand is usually in a pronated or palm down position. Tearing or rupture of the TFCC occurs when there is enough force through the ulnar side of the hyperextended wrist to overcome the tensile strength of this structure.
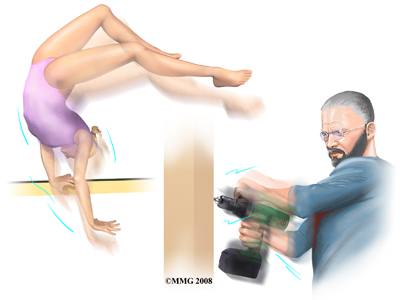
High-demand athletes such as tennis players or gymnasts (including children and teens) are at greatest risk for TFCC injuries. TFCC injuries in children and adolescents occur more often after an ulnar styloid fracture that doesn't heal. Power drill injuries also often cause TFCC rupture when the drill binds and the wrist rotates instead of the drill bit. TFCC tears can also occur with degenerative changes. Repetitive pronation (palm down position) and gripping with load or force through the wrist are risk factors for tissue degeneration. Degenerative changes in the TFCC structure also increase in frequency and severity as we get older; thinning soft tissue structures that occur with age can result in a TFCC tear with minor force or minimal trauma.
There may be some anatomical risk factors for TFCC injuries. Studies show that patients with a torn TFCC often have ulnar variance and a greater forward curve in the ulnar bone. Ulnar variance means the ulna is longer than the radius because of congenital (present at birth) shortening of the radius bone in the forearm.
Symptoms
What does the condition feel like?
Wrist pain along the ulnar side is the main symptom. Some patients report diffuse pain, which means the pain is throughout the entire wrist area and can't be pinpointed to one area. The pain is made worse by any activity or position that requires forearm rotation and movement in the ulnar direction. This includes simple activities like turning a doorknob or key in the door, using a can opener, or lifting a heavy pan or carton of milk with one hand.
Other symptoms include swelling, clicking, snapping, or crackling (called crepitus) and weakness of the wrist. Some patients report a feeling of instability, like the wrist is going to give out on them. Others report that it is as if something is catching inside the joint. There is usually tenderness on palpation along the ulnar side of the wrist.
In cases of a traumatic injury a fracture needs to be ruled out. If a fracture at the wrist end of the ulna bone is present along with soft tissue instability, then forearm rotation may be very limited. The direction of limitation (palm up or palm down) depends on which direction the fractured portion of the ulna dislocates.
Diagnosis
How do health care professional diagnose the problem?
Diagnosis begins with a complete history of your injury. Your physical therapist at Optimum Recovery Rehab Physical Therapy & Rehabilitation will ask questions about where precisely the pain is, when the pain began, if there was a specific injury that occurred or whether the pain gradually developed over time, and what movements aggravate or ease the pain. They will also ask if there is any swelling, clicking, catching, or weakness in the wrist.
Next they will do a physical examination. Your therapist will palpate all around the wrist to determine your most tender point. They will also look for swelling or redness in the area. Next they will check the strength of your muscles around the wrist, elbow, and hand. They will ask you to resist certain movements while checking for pain as well as strength deficits. They may also do a grip strength test to determine if your injury has caused you to lose some of your strength and to get a baseline measure so they can easily track your improvement with rehabilitation.
Other tests may be done to provoke the symptoms and test for excess or restricted movement at the wrist. These tests include hypersupination (overly rotating the forearm in a palm-up position), loading the wrist in a position of ulnar deviation (moving wrist away from the thumb), and passively putting the wrist into a fully extended position.
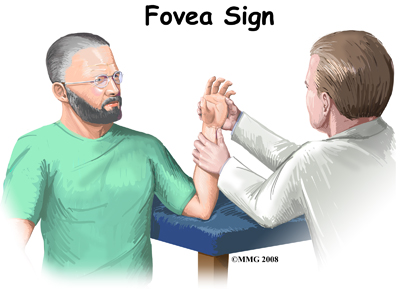 A new test called the fovea sign applies external pressure to the area of the fovea on the ulna bone. The examiner compares the involved wrist with the normal wrist. Tenderness and pain during this test is a sign that there may be a split-tear injury (down the middle length-wise) of the TFCC.
A new test called the fovea sign applies external pressure to the area of the fovea on the ulna bone. The examiner compares the involved wrist with the normal wrist. Tenderness and pain during this test is a sign that there may be a split-tear injury (down the middle length-wise) of the TFCC.
Split tears are more common with lower energy, repetitive torque injuries such as from bowling or golfing. This type of ligament injury was first discovered when a surgeon pushed on the area of pain while using an arthroscope to look inside the joint. When the surgeon did this he saw the ligament open up like a book.
X-rays may show disruption of the TFCC when there is a bone fracture present, however ligamentous instability without bone fracture appears normal on standard X-rays. An X-ray with a dye injected is called a wrist arthrography. Arthrography is positive for a TFCC tear if the dye as seen on X-ray leaks into any of the joints. During this test there are three specific joint areas tested, so this test is called a triple injection wrist arthrogram.
Acute injuries can be painfully swollen preventing proper physical examination. In such cases, more advanced imaging such as MRIs can be used to detect ligamentous or other soft tissue damage. MRIs can be useful to detect TFCC injuries even without dye injected. When the MRI is done with a dye injected into the area, however, the test is called an MRI arthrogram. If the dye moves from one joint compartment to another, a tear of the soft tissues is suspected. Unfortunately studies show that almost half the patients with a true TFCC tear have normal arthrograms.
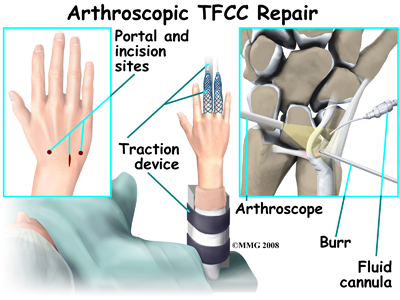
Wrist arthroscopy is really the best way to accurately assess the severity of damage with a TFCC injury. At the same time as assessing the TFCC, the surgeon performing the arthroscope looks for other associated injuries of related ligaments and cartilage. The surgeon performs the arthroscope by inserting a long thin needle into the joint. A tiny TV camera on the end of the instrument allows the surgeon to look directly at the tissues of the joint.
Using a probe, the surgeon tests the integrity of the soft tissues. A special trampoline test can be done to see if the fibrocartilage disk is okay. During this test the surgeon presses the center of the disk with the probe. Good tension and an ability for the tissue to bounce back shows that the disk is attached normally and is not torn or damaged. If the probe sinks, as if on a feather bed, the test is positive (indicating a tear). One advantage of an arthroscopic exam is that treatment can often be done at the same time.
An accurate diagnosis and grading of the injury (degree of severity) is important. There are two basic grades of triangular fibrocartilage complex injuries. Class 1 is for traumatic injuries. Class 2 is used to label or describe degenerative conditions. Usually, the grade is based on how much disruption of the ligament has occurred (minimal, partial, or complete tear).
Optimum Recovery Rehab Physical Therapy & Rehabilitation provides services for physical therapy in West Orange.
Treatment
What treatment options are available?
Nonsurgical Treatment
If the wrist is still stable, then conservative (non-operative) care is advised. You may be given a temporary splint to wear for four to six weeks. The splint will immobilize (hold still) your wrist and allow scar tissue to form at the injury site. Anti-inflammatory drugs may be prescribed and physical therapy will be recommended. You may benefit from one or two steroid injections spaced apart by several weeks.
If the wrist is unstable but you don't want surgery, then your doctor may put a cast on your wrist and forearm. In some cases it is possible to use a splint for six weeks instead of casting, and to start physical therapy once the immobilization period is over.
With appropriate non-surgical treatment and adherence to a rehabilitation program at Optimum Recovery Rehab Physical Therapy & Rehabilitation many patients with a mild triangular fibrocartilage complex injury are able to return to work and/or sports at a preinjury level. Pain-free movement and full strength are possible.
Non Surgical Rehabilitation
The initial aim of treatment for a TFCC injury at Optimum Recovery Rehab Physical Therapy & Rehabilitation will be to decrease the inflammation and pain around the area. Simply icing your wrist assists with the inflammation and often relieves a great deal of the pain. In cases of more chronic pain, heat may be more useful. Your physical therapist may also use electrical modalities such as ultrasound or interferential current to help decrease the pain and inflammation. Massage for the muscles of the forearm may also be helpful at this stage.
As many wrist motions easily aggravate this injury it is important to stop or change any activities that are causing symptoms. If possible, your therapist will encourage you to avoid repetitive hand motions such as heavy grasping, wringing, as well as turning and twisting movements of the wrist. Lifting objects with one hand should also be avoided. If it is unavoidable to use your hand, then taking frequent breaks during activity is a must.
In addition to giving the wrist as much rest as possible, keeping your wrist in a neutral alignment will also assist in the healing process. In other words, keeping it in a straight line with your arm, without bending it up or down or twisting it. You may have already used a splint suggested by your doctor, but if not, your physical therapist may suggest you start using one. Tape or strapping can sometimes be an alternative to a splint, or can be used in addition to one. Tape, however, is not as sturdy as a splint so generally does not provide as much relief or as optimal of a healing environment as a rigid brace. That being said, tape may be a useful alternative for when full immobilization of the wrist is not feasible.
As part of your treatment your physical therapist may check your workstation posturing and the way you do your daily tasks. We will also educate you about healthy body alignment and proper wrist positions. It is our belief at Optimum Recovery Rehab Physical Therapy & Rehabilitation that preventing future problems is as much a part of our treatment as treating the current injury.
Once the initial pain and inflammation has calmed down, your physical therapist will focus on improving the mobility and strength of your wrist and hand. They will take measurements of your wrist range of motion and grip strength to determine if there are any specific deficits to work on and to track your progress.
Simple wrist and finger stretching exercises will be prescribed and should be done within the limits of pain. Exercises to improve the motions of bending and straightening of the wrist, turning your palm up (supination) and then back over (pronation,) moving your wrist towards your little finger (ulnar deviation) and then towards your thumb (radial deviation), as well as twisting of the wrist will be given.
Strengthening exercises will also be prescribed. These exercises will focus on improving both the strength of the wrist as well as the ability of the hand to grip and exert force when twisting, grabbing, bearing weight, or doing functional activities such as those required for your work or sport. Exercises to improve strength will include eccentric exercises for the forearm muscles. Eccentric contractions occur as the muscle lengthens and the tendon and muscle is put under stretch. Eccentric exercises for the wrist are initiated by dropping the wrist down slowly at first and then also slowly returning to the neutral position. As able, the drop portion of the exercise is progressed to a quick motion. These exercises will help to build up the tensile strength in the tissues and associated muscles of the wrist to be able to control and protect the wrist. Strengthening exercises will be prescribed not only for the bending motion of your wrist, but also for the motion where your wrist moves towards and away from your thumb (ulnar and radial deviation.) This motion, along with rotation of the wrist, are particularly stressful to the TFCC area. Your therapist will ensure that your injury is at an appropriate stage of healing before introducing eccentric exercises or strengthening ulnar and radial deviation as these types of exercises put significant stress through the TFCC area and can aggravate a healing injury. Another stressful exercise for the tissues of the TFCC is one that involves putting weight-bearing force through the wrist, such as when you push a door open with your hand, or do a push up. Your therapist will add these types of exercises once they know the healing process has progressed enough to not aggravate your wrist. These exercises should begin in a neutral position (such as the position you would use when making a fist) and progress to a position where weight is being put through the wrist while it is extended (such as a wall or floor push up position).
Therapeutic tools such as elastic putty or gripping balls might be used to add resistance for your wrist. As you become stronger, weights or resistance bands will be used to further build up strength. Fine motor control and dexterity exercises for your thumb and hand may also be added into your rehabilitation routine depending on your occupation or the cause of your injury. Your therapist may ask you to do daily functional tasks such as fold the laundry, twist door handles, or unload the dishwasher as part of your therapy. These exercises force the wrist to do combined motions such as rotation and extension, and stress the tissues of the TFCC in ways similar to how it is stressed during everyday activities.
Proprioception is the ability for you body to know where it is in space without looking at it. With any injury, this ability declines. A period of immobilization adds to this decline. Without proper proprioception any joint is at an increased risk of injury. Your therapist will prescribe exercises to address proprioception of your wrist. The may ask you to roll a ball with your hand against a wall or gently toss and catch a light ball. Many advanced exercises for strength also incorporate proprioception.
Residual laxity may remain after nonoperative treatment of a TFCC injury. If conservative care is unsuccessful, persistent joint laxity and instability can lead to degeneration of the joint’s articular cartilage. Too much force or compression on either side of the joint can lead to pain and altered movement patterns. If non surgical treatment is not effective then surgery may be needed to restore normal wrist movement.
Optimum Recovery Rehab Physical Therapy & Rehabilitation provides services for physical therapy in West Orange.
Surgery
Surgical treatment is based on the specific injury present. Instability as a result of a complete ligamentous rupture, especially with a bone fracture, requires surgery as soon as possible.
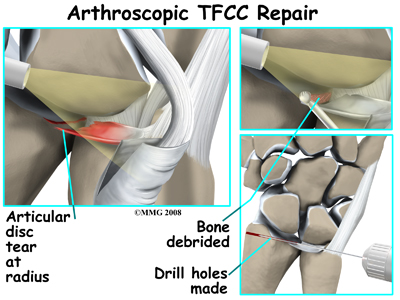
 The outside perimeter of the TFCC has a good blood supply. Tears in this area can be repaired. There is no potential for healing when tears occur in the central area where there is no blood supply. In these cases arthroscopic debridement of the damaged tissue is required.
The outside perimeter of the TFCC has a good blood supply. Tears in this area can be repaired. There is no potential for healing when tears occur in the central area where there is no blood supply. In these cases arthroscopic debridement of the damaged tissue is required.
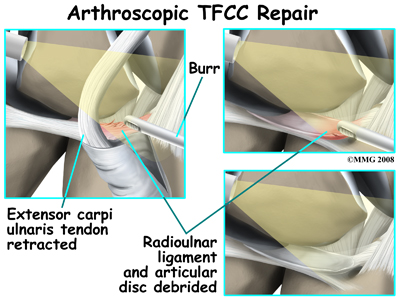
During arthroscopic debridement the surgeon smooths or shaves any tears of the disc or meniscal homologue that might catch against the joint surfaces. The surgeon then looks for any problems with the foveal ligament. A probe is used to detect tension or laxity (looseness) of the ligaments. Laxity is a sign of injury.
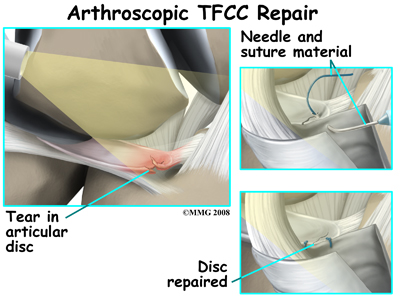
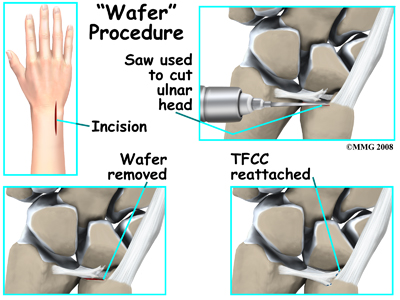
Arthroscopic debridement works well for simple tears. Much of the damaged tissue can be removed while still keeping a stable wrist joint. The torn structures can be reattached with repair sutures. Some surgeons perform an arthroscopic wafer procedure (see below) in addition to the TFCC debridement especially when both TFCC disruption and positive ulnar variance are present. Further studies are needed to see if the combined procedure results in a more satisfactory outcome than current methods and to evaluate the rotational loss that can occur with this combined procedure.
Some ligamentous ruptures with a fracture can also be repaired arthroscopically with reattachment and instrumentation. Instrumentation refers to the use of hardware such as wires and screws to help hold the repaired tissue in place until healing occurs.
Although they are not common, there are some complex tears that require open repair. Open repair means the surgeon makes an incision and opens the tissues to perform the operation. This gives the surgeon a better view and better access of the area. The specific procedure required depends on the tissues injured and the extent of the injury. For example, detachment of the radioulnar ligaments usually requires open repair. Instability of the distal radioulnar joint may require the use of wires to hold the area together until healing occurs. In other cases, surgery has been delayed so long that the torn ligament has retracted (pulled back) too far and a direct repair can't be done. In these cases, a tendon graft may be needed to help strengthen the repair.
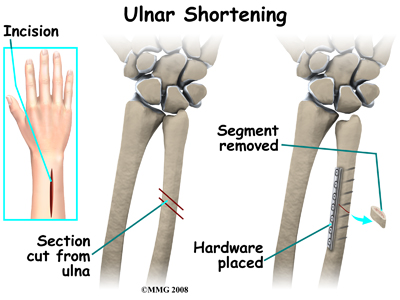
Chronic and degenerative TFCC tears may require a different surgical approach. Debridement is not as successful with this group as it is with acute TFCC injuries. Sometimes it is necessary to shorten the ulnar bone at the wrist to obtain pain relief. There are two procedures used to shorten the ulna and unload the ulnocarpal joint. These are the ulnar (diaphyseal) shortening method and the distal ulnar head shortening osteotomy (Feldon wafer method). If lunate-triquetrum instability is present, ulnar shortening can be done to tighten the ulnocarpal ligaments and decrease the motion between the lunate and triquetrum.
When making the decision as to which procedure to use the surgeon weighs the amount of shortening needed and the structure of the distal radioulnar joint, which will affect the joint loading.
With the diaphyseal shortening method (using internal fixation - plate/screws) there is a higher complication rate (ie. delayed union, nonunion, hardware removal).
Distal ulnar head shortening osteotomy (ie. Feldon wafer method) is an arthroscopic or open method (only 2-3mm of shortening.) It is less invasive and provides equal relief to diaphyseal shortening.
After Surgery
Your wrist will be immobilized in a bulky dressing or cast. The type of immobilizing device used and the position your wrist is placed in depends on the type of surgery you had. Your surgeon may encourage simple finger and elbow motions soon after surgery.
Pain relief, improved motion, and increased function are the main goals of surgery for most patients. The surgeon is also interested in restoring wrist stability and the load bearing function of the wrist. After the initial soreness from the surgery is gone, you should experience a significant decrease in pain. Many patients report being pain free.
The follow-up plan after surgery may vary depending on the type of procedure used by your surgeon. Newer and improved methods have made it possible for some patients to return to full, unrestricted activity as early as six weeks post-op.
The standard surgery usually follows a typical course. One week after surgery, the splint will be replaced with a fiberglass type cast (still in a supinated position). The elbow is left free to move fully. The cast will be removed six weeks after the operation. Cast removal is followed by physical therapy for six to eight weeks.
Rehabilitation
What should I expect after surgery?
Rehabilitation at Optimum Recovery Rehab Physical Therapy & Rehabilitation will begin as soon as your surgeon allows it. Each surgeon will set his or her own specific activity restrictions based on the surgical procedure used, their personal experience, and whether or not wrist is healing as expected.
Even while the cast is on and before extensive physical therapy begins, at Optimum Recovery Rehab Physical Therapy & Rehabilitation we highly recommend maintaining the rest of your body’s fitness with regular exercise. Activities such as walking or using a stationary bike or stepper machine are easy activities that can be done even while the wrist is healing. Avid runners may be able to continue running with clearance from their doctor. Weights or weight machines for your lower extremity and opposite arm are also acceptable to use as long as the restrictions regarding your healing wrist are strictly abided by. Lifting any weight at all with your injured side will not be allowed while your wrist is in the initial healing stages so you may require a friend to assist you with your workout if you are keen to continue during this time. Your physical therapist at Optimum Recovery Rehab Physical Therapy & Rehabilitation can discuss the most appropriate way for you to maintain your fitness while abiding by your doctor’s restrictions, and can provide a general fitness program specific to your needs.
When the cast is first removed after surgery you may experience some pain when you start to move your wrist, elbow and forearm. This pain is from not using the joints regularly while your wrist has been immobilized as well as from the surgical process itself. Your physical therapist at Optimum Recovery Rehab Physical Therapy & Rehabilitation will focus initially on relieving this pain. They may use modalities such as heat, ice, ultrasound, or electrical current to assist with decreasing any pain or swelling you have around the wrist or anywhere along the arm or into the hand. In addition, they may massage the hand, forearm, wrist, or elbow to improve circulation and assist with pain.
The next part of your treatment will focus on regaining the range of motion, strength, and dexterity in your wrist, hand, elbow, and shoulder. Your physical therapist at Optimum Recovery Rehab Physical Therapy & Rehabilitation will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of a home exercise program. These exercises may include the use of rehabilitation equipment such as pliable balls, exercise bands, or small weights that provide added resistance for your hand and wrist. Your physical therapist may even give you exercises for your shoulder. The shoulder is the link of the upper limb to the rest of the body so it needs to be strong and well controlled for the upper extremity, particularly the wrist and hand, to work well. In addition, compensatory motions of the shoulder can affect how you use your wrist and lead to secondary pain in your shoulder.
The initial exercises prescribed will not require you to put any of your body weight through the wrist; you may simply be moving the wrist back and forth, side to side, turning your palm up and down, and rotating your wrist within the limits of pain. As your healing wrist allows, your physical therapist will add in exercises where you are putting more stress through the wrist by taking the wrist into full ranges of motion, doing quick wrist motions, and doing eccentric strength exercises (see description under non-surgical rehabilitation). At the appropriate time your therapist will add in exercises where you are putting some of your body weight through your wrist via your hand, such as when pushing on a door or doing push ups against a wall.
Some patients have difficulty regaining pinch grip and grip strength after TFCC surgery so this will be addressed with specific exercises. Your therapist at Optimum Recovery Rehab Physical Therapy & Rehabilitation will also focus particularly on gaining back those ranges of movement which are commonly lost after this type of surgery. These include ulnar deviation, supination, pronation, and wrist extension.
If necessary, your physical therapist will mobilize your joints in order to gain range of motion. This hands-on technique encourages any stiff joints in your wrist, hand and elbow to move gradually into their normal range of motion.
As a result of any injury, the receptors in your joints and ligaments that assist with proprioception (the ability to know where your body is without looking at it) decline in function. A period of immobilization will add to this decline. Although your wrist is not traditionally thought of as a weight-bearing joint, even activities such as pushing up to get off of the couch, pulling a glass from a cupboard, or pushing a door open, require weight to be put through or lifted by your wrist and for your body to be proprioceptively aware of your limb. If you are active in sport, then proprioception of your upper extremity is paramount in returning you to your sport after surgery for a TFCC injury. Your physical therapist at Optimum Recovery Rehab Physical Therapy & Rehabilitation will prescribe exercises for you to regain this proprioception. These exercises may include activities such rolling a ball on a surface with your hand, holding a weight up overhead while moving your shoulder, or lightly tossing an item up and catching it. Advanced exercises wil
l include exercises such as ball throwing or catching overhead.
Fortunately, gaining range of motion, strength, and proprioception after surgery for a TFCC injury occurs fairly quickly. You will notice improvements in the functioning of your wrist even after just a few treatments at Optimum Recovery Rehab Physical Therapy & Rehabilitation. As you improve, we will advance your exercises to ensure your rehabilitation is progressing as quickly as your healing wrist allows. Once your wrist can tolerate it, advanced exercises may include activities such as holding a push up position with your hands on a basketball, or dips in a chair where you are taking nearly your whole body weight through your wrist. It is crucial at each stage of rehabilitation to closely follow the instructions of your physical therapist as the TFCC area can be easily aggravated if too much is done too quickly.
Generally, the wrist responds very well to the physical therapy we provide at Optimum Recovery Rehab Physical Therapy & Rehabilitation after surgery for a TFCC injury. Many patients are able to return to work with no restrictions. A small number of patients may require some work restrictions or permanent changes in work tasks. It should be noted, however, that in some cases complications such as persistent pain and stiffness occur. Your therapist will ask you to follow-up with your doctor if they feel your rehabilitation is not progressing as it should. Other complications such as infections, delayed union, or nonunion of bone fractures may also be a problem. In some cases further surgery may be needed to revise the first operation. Some patients need another surgery to remove any hardware used to stabilize the joint. In other cases the bottom of the ulna called the styloid may have to be removed. In rare cases, the procedure fails to provide the desired results and a wrist fusion may be the next step.
Portions of this document copyright MMG, LLC.
Optimum Recovery Rehab Physical Therapy & Rehabilitation provides services for physical therapy in West Orange.